By Rafael Chavez, MD
A 23 yo male is brought into the resus booth by EMS with multiple GSWs to the chest and abdomen. He arrives hypotensive, tachycardic, GCS of 3, and is being bagged by EMS with an O2 sat of 89%. While your senior starts running the trauma, they ask you to intubate the patient. Using direct laryngoscopy, you are unable to visualize the vocal cords and see nothing but blood in the airway. As you start to suction, the patient’s O2 sat quickly drops to 60%, he becomes bradycardic, and arrests. With the laryngoscope still in place, you try to pass the bougie blindly into the pool of blood but can tell it just keeps going into the stomach. With the thoracotomy in progress, you quickly reassess the situation and think about what to do next: What airway options do I have left? Should I do a surgical cricothyroidotomy? How do I cric again? Do I have a change of underwear in my car?
Let’s review the uncommon ED procedure of the emergent cricothyroidotomy: The cricothyroidotomy comes in two flavors: surgical and needle. The needle cricothyroidotomy is done in children less than 8 years old. Equipment In a pinch all you really need is the following:
- 11 blade scalpel
- Bougie
- 6.0 cuffed ET tube or tracheostomy tube (i.e. Shiley 6.0)
- 10 cc syringe
Or you can just get a cricothyroidotomy kit with a tracheostomy tube.
**Anatomy **Recall the location of your cricothyroid membrane between the thyroid cartilage and the cricoid cartilage.
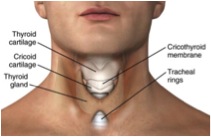
Roberts and Hedges’ Clinical Procedures in Emergency Medicine, Chapter 6, p120-133 (Figure 6-1)
Procedure instructions:
Check out our Cricothyroidotomy Blog PDF with step-by-step instructions, tips, and resources
You quickly decide the patient needs a surgical airway. Being a well-prepared resident, you already have a #11 blade in your pocket. While getting into position, you ask the RT to load a 6.0 ET tube onto a bougie. With your left hand firmly holding the thyroid cartilage, you located the cricothyroid membrane via landmarks and make your first incision vertically through the skin. The neck begins to bleed profusely but you are able to palpate the cricothyroid membrane with your free left index finger and make a **horizontal **incision through it. There is a rush of blood filled air onto your facemask but find the hole through the membrane with your finger. You successfully pass the bougie along your finger into the trachea and then finally the ET tube. The airway is now secured and the patient’s O2 sat slowly rises to 99%. A few minutes later after open chest CPR, cross clamping the aorta and 2 units of blood, the patient gets a pulse back and is transferred to the OR for further management.